

OPINION: SHA/SHIF - Let’s dream a little, shall we?

File image of the SHA buildings in Nairobi. PHOTO | COURTESY

Audio By Vocalize

By
Paulie Mugure Mugo
Here’s
the dream:
A
young boy - let’s call him Justus - leaves his modest home somewhere in Kibra and
heads to a nearby compound a few meters down the road. He is carrying a yellow
ten-liter jerrycan, having been sent to the landlord’s home to fetch water
for his family’s needs.
But
as he hops playfully along, exchanging boyish banter with his neighborhood
pals, Justus suddenly finds himself smack in the path of a speeding
motorbike. Thwack! The violent thrust of hard steel against
the young boy’s tender frame leaves Justus lying motionless on the road,
jerrycan hurled several meters away and his thigh bone broken in two.
Screams
rent the air as a crowd gathers rapidly. In the ensuing melee, the motorbike
scampers off in a quick minute.
Meanwhile,
a sharp-witted neighbor recognizes the injured boy; she grabs her phone, dials
a four-digit number and an ambulance shortly arrives. Justus is whisked off to
the nearest suitable hospital, where he is admitted and treated carefully for
the next three months. Due to the seriousness of his injury, the hospital bill
quickly builds up, but his widowed mother is spared the indignity of begging
for help when his Ksh.300,000 bill is promptly settled courtesy of government
coffers.
End
of dream.
Believe
it or not, ladies and gentlemen, such an incident was narrated to me some days
ago by a lady named Mary*, an industrious, widowed mother of five who happens
to be Justus’ real-life mum. But her version didn’t end quite so well.
You
see, one afternoon in November 2019, Mary, who was employed as a househelp at
the time, had just finished frying chapatis for her bosses’ lunch, when her
mobile phone rang.
“Mary, kuja Mbagathi,” the caller had yelled
urgently. “Kimbia haraka..!”
On
the line was her neighbor, a friendly lady whose vegetable stall was just a few
meters from Mary’s Kibra home. Unbeknownst to Mary, little Justus, her
9-year-old son, had been heading to their landlord’s compound to fetch water,
when he had been slammed violently to the ground by a speeding boda boda. It
had been about half an hour since the incident occurred and the boy was now at
the Mbagathi County Referral Hospital. Mary pleaded with her neighbor to share
more details.
“Kimbia Mbagathi tu,” was the response; and no
one else, it seemed, was willing to explain what exactly had happened. So, the
terrified mother quickly downed her tools and ran to her son.
Mbagathi
Hospital, where young Justus had been rushed, is one of about 47 county
referral facilities located across Kenya and is managed by the county
government of Nairobi. Commissioned in 1956 by Sir Fredrick Crawford - the
deputy governor of Kenya at the time - Mbagathi was for a long time known as
Infectious Diseases Hospital (IDH), due to its initial role as an isolation
facility for the Kenyatta National Hospital (KNH). Having provided treatment
for diseases such as tuberculosis
and meningitis for almost fifty years,
the hospital began the transition to a fully-fledged district-level hospital in
1995. It is now one of Nairobi’s major referral facilities, handling almost
1,000 outpatient cases daily and boasting an inpatient capacity of 320 beds.
Kenya’s
healthcare system categorizes medical facilities from Level 1 to Level 6.
Mbagathi ranks at Level 5 and offers the wide range of services expected at
that level. So, when Mary got to the hospital that Saturday afternoon, she
found that an X-ray had already been done, revealing that her son’s left femur had been broken in two and that the lower
piece had moved a couple of inches upwards, with a portion of it lying parallel
to the other.
As
soon as the accident had occurred, Mary learned, a crowd had gathered rapidly
around her son, placed him hurriedly on a passing motorbike, and rushed him to
Mbagathi Hospital. That’s when she received that chilling call. But the good
Samaritans’ actions, while well-intentioned, had in all probability worsened the
condition of the child’s broken bone.
“Ilikuwa imeshikana hivi,” Mary
told me, folding her arms in front of her, each arm touching the other, with
one placed a few inches lower.
The
two pieces of bone would now have to be pulled apart and repositioned carefully
via skeletal traction, a contraption that combines pulleys, pins, and weights
to treat broken bones. Mary was advised that an urgent transfer to the Level 6
Kenyatta National Hospital was necessary.
Thus,
mother and son began a journey that would stretch two full months and eighteen days and leave Mary indebted in
the staggering amount of Ksh.257,944. It was more money than she had ever seen.
In
the almost 80 days that Justus lay at KNH, his leg strung up and strictly stationary, several hospital
staff inquired if anyone had captured details of the offending motorbike,
hoping, perhaps, to help bring its rider to
book.
But
in the crucial moments after the crash, the only thing that Mary’s kind
neighbor - and main witness - had seen, were the retreating backs of the boda
driver and his passenger, as they scrambled hastily off the ground, jumped back
on the motorbike and fled. And no one who had been in the crowd that day had
anything further to add. So, there was no hope of any kind of recompense from
that end.
Mary’s
monthly salary was Ksh.10,000 at the time and the last time she had contributed
to NHIF was six years earlier, when she had been formally employed by a
mid-sized trading company. Needless to say, she had no private insurance either.
So, the formidable buck stopped squarely at her work-worn feet.
“Plead
your case to a social worker at KNH,” someone advised when her son’s discharge
date drew near, suggesting that she garnish her story with tearful wails, if
necessary. “Toa machozi,” he
said.
So,
in anticipation of pleading for her son’s release, the desperate mother had
sought every single person or group willing to donate funds that she could
present to KNH as her contribution to the huge debt. Her plan was to humbly
request the hospital, through the good offices of their social workers, to
write off the balance once she paid part of the bill.
So,
at her request, Mary’s church kindly conducted a mini fund-raiser; Justus’
Kibra-based primary school chipped in; and her friends, family, and employer
gave what they could. Altogether, they were able to raise Ksh.30,000. And on
the day that she was to settle her son’s bill, Mary tucked the cash tightly
into her purse and made her way to the hospital dressed in her oldest and most
tattered clothes, hoping that her miserable appearance might aid her plea. To
her great relief, upon the recommendation of the social worker, the hospital
accepted the Ksh.30,000, and her child was discharged.
As
the debate on the recently launched Social Health Authority (SHA) has continued
to rage, I have been reminded of this story related to me by Mary, who now
works in my home. The truth is that, like Mary, the majority of households
in Kenya simply cannot afford to cater for the prolonged hospitalization of a
loved one; many could quite easily find themselves suddenly impoverished by the
critical illness of even one member of the family. We all
know what it means when we unexpectedly find ourselves in a WhatsApp group
named “Mary’s Medical Fund”, for example. Just a few days ago,
I found myself in one such group, having been roped in by an individual I last
saw in 2017.
So, now that NHIF, Kenya’s former national insurance, has been
put to bed and is resting quietly in peace, I thought I might as well educate
myself on the new, hotly-debated SHA.
The
concept of affordable, quality healthcare for all has been a long-held
aspiration for our country and was identified as a key priority in our Vision
2030 strategic plan. Accordingly, a number of initiatives have since been
established in an effort to strengthen healthcare provision in Kenya.
President Uhuru Kenyatta, for example, incorporated Universal
Health Coverage (UHC) as part of his administration’s Big Four Agenda. And in
December 2018, the former president launched a pilot UHC scheme in four counties
namely Kisumu, Isiolo, Nyeri and Machakos, and subsequently kicked off a
roll-out of the same to the other counties in February 2022.
But the current effort to attain UHC through the SHA, while
building on previous initiatives, represents the most aggressively ambitious
attempt yet.
The Social Health Authority (SHA), established in October 2023, aims to deliver UHC through three distinct funds, two of which will provide essential healthcare services free of charge to the Kenyan populace. These are the Public Healthcare Fund (PHC) and the Emergency, Chronic & Critical Illness Fund (ECCIF).

Through
the ECCIF, SHA aims to provide emergency services for all, such as accident,
critical illness and ambulance services. One can’t help but imagine that if an
ambulance had been available for young Justus, he may have been spared the
improper handling he suffered at the hands of eager but unskilled good
Samaritans that had very likely exacerbated his injury.
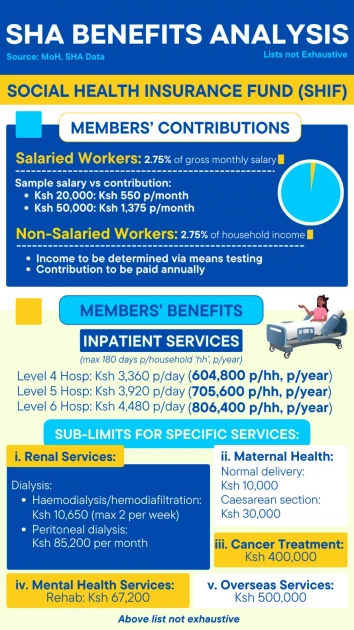
The
third fund is the Social Health Insurance Fund (SHIF), and contribution to this
is mandatory for all Kenyans at 2.75% of household income. This will be paid
either on a monthly basis by salaried employees, or on an annual basis by all
others. The minimum contribution will be Ksh.300 per month.
SHIF
will entitle paid-up households to a raft of services such as enhanced
outpatient services, medical imaging, maternal care, renal care, cancer
management, surgery and more.
Access
to inpatient services will be at Ksh.4,480 per day in Level 6 hospitals such as
Kenyatta Hospital, Moi, Kisii and Meru Teaching and Referral Hospitals, among
others. Theoretically,
had Mary been a member of SHIF and contributed the minimum Ksh.300 per month
commensurate with her salary, Justus’ Ksh.257,944 bill at KNH would easily have
been settled. Since SHIF caters for inpatient care for a maximum of 180 days
per household, per year, a good amount of cover would still have been left
available in case of any other hospitalization that year.
A survey of private Level 5 hospitals such as Mater Misericordiae, AAR Hospital, the Aga Khan and Nairobi Hospital shows that the general ward bed charges range from Ksh.8,200 to upwards of Ksh.11,000 per day. The SHIF contribution to this is set at Ksh.3,920 per day which is close to what NHIF formerly paid for similar facilities. Like its predecessor, SHA does not bar members from acquiring additional cover from private insurance companies to cover charges that may exceed its set limit.
Not
many nations worldwide have achieved truly successful universal health
coverage, and there have been undeniable challenges in the roll-out of our home-grown
SHA. Some issues may even persist for some time. However, I find myself
persuaded that, if properly implemented, SHA represents a huge leap forward in
healthcare provision for our country. And so, in the last few days, in hopeful
anticipation of better days, I have ensured that my entire household, and
Mary’s, have been registered with the SHA. We’re an optimistic lot around here.
In
October last year, when President William Ruto assented to four parliamentary
bills that paved the way for the implementation of SHA’s scheme, he stated
that as a country we had “reached a pivotal moment in our quest to reshape our
healthcare”, and that we now had a firm foundation for “the biggest change in
our healthcare system ever witnessed.”
I
am hopeful that his government will deliver on this promise, and that I will
not be forced to swallow this 2,185-word ode to hope. Nevertheless, I choose to
keep my indigestion tabs close by, just in case. And my 2027 vote.
Meantime,
I choose to dream.
*Names
have been changed.
[Paulie
Mugure Mugo is a published author and a co-founder of Eagles Leadership Network
(ELN), an initiative that trains and equips upcoming leaders in the area of
ethical governance.]
Leave a Comment